136 reads in the past 30 days
Research trends of artificial intelligence in pancreatic cancer: a bibliometric analysis



August 2022
·
2,893 Reads
·
14 Citations
Published by Frontiers
Online ISSN: 2234-943X
Disciplines: Geriatrics and Gerontology
136 reads in the past 30 days
Research trends of artificial intelligence in pancreatic cancer: a bibliometric analysisAugust 2022
·
2,893 Reads
·
14 Citations
134 reads in the past 30 days
Double osseous flaps for simultaneous midfacial and mandible reconstruction: Automation in surgical complexity within an entirely computerized workflowFebruary 2023
·
697 Reads
125 reads in the past 30 days
Three-Dimensional 3D Culture Models in Gynecological and Breast Cancer ResearchMay 2022
·
1,105 Reads
·
11 Citations
115 reads in the past 30 days
Mycosis fungoides and Sézary syndrome: clinical presentation, diagnosis, staging, and therapeutic managementApril 2023
·
290 Reads
·
11 Citations
98 reads in the past 30 days
Deep Learning Model for Classifying Metastatic Epidural Spinal Cord Compression on MRIMay 2022
·
1,381 Reads
·
13 Citations
Frontiers in Oncology is a broad-scope, multidisciplinary journal covering all areas of cancer research to advance our knowledge of cancer epidemiology to improve diagnosis, therapeutics and management strategies.
Led by Field Chief Editor Prof Giuseppe Giaccone (Cornell University, USA, and Amgen), and Assistant Field Chief Editor Prof Sharon Pine (University of Colorado, USA), Frontiers in Oncology welcomes clinical and experimental research contributions in the various domains of cancer research, which bridge the gap between basic research and clinical applications. Topics include, but are not limited to:
Manuscripts consisting solely of bioinformatics, computational analysis, or predictions of public databases which are not accompanied by validation (independent clinical or patient cohort, or biological validation in vitro or in vivo, which are not based on public databases) are not suitable for publication in this journal.
Frontiers in Oncology is committed to advancing developments in the field of cancer research by allowing unrestricted access to articles, and communicating scientific knowledge to researchers and the public alike, to enable the scientific breakthroughs of the future.




May 2024
·
2 Reads
 Guotian Pei
Guotian Pei
·
Kunkun Sun
·
Yingshun Yang
·
[...]
·
Yuqing Huang
Background Multiple primary lung cancer (MPLC) is an increasingly well-known clinical phenomenon. However, its molecular characterizations are poorly understood, and still lacks of effective method to distinguish it from intrapulmonary metastasis (IM). Herein, we propose an identification model based on molecular multidimensional analysis in order to accurately optimize treatment. Methods A total of 112 Chinese lung cancers harboring at least two tumors (n = 270) were enrolled. We retrospectively selected 74 patients with 121 tumor pairs and randomly divided the tumor pairs into a training cohort and a test cohort in a 7:3 ratio. A novel model was established in training cohort, optimized for MPLC identification using comprehensive genomic profiling analyzed by a broad panel with 808 cancer-related genes, and evaluated in the test cohort and a prospective validation cohort of 38 patients with 112 tumors. Results We found differences in molecular characterizations between the two diseases and rigorously selected the characterizations to build an identification model. We evaluated the performance of the classifier using the test cohort data and observed an 89.5% percent agreement (PA) for MPLC and a 100.0% percent agreement for IM. The model showed an excellent area under the curve (AUC) of 0.947 and a 91.3% overall accuracy. Similarly, the assay achieved a considerable performance in the independent validation set with an AUC of 0.938 and an MPLC predictive value of 100%. More importantly, the MPLC predictive value of the classification achieved 100% in both the test set and validation cohort. Compared to our previous mutation-based method, the classifier showed better κ consistencies with clinical classification among all 112 patients (0.84 vs . 0.65, p <.01). Conclusion These data provide novel evidence of MPLC-specific genomic characteristics and demonstrate that our one-step molecular classifier can accurately classify multifocal lung tumors as MPLC or IM, which suggested that broad panel NGS may be a useful tool for assisting with differential diagnoses.
May 2024
·
4 Reads
Stress-induced promoter-associated and antisense lncRNAs (si-paancRNAs) originate from a reservoir of oxidative stress (OS)-specific promoters via RNAPII pausing-mediated divergent antisense transcription. Several studies have shown that the KDM7A divergent transcript gene ( KDM7A-DT ), which encodes a si-paancRNA, is overexpressed in some cancer types. However, the mechanisms of this overexpression and its corresponding roles in oncogenesis and cancer progression are poorly understood. We found that KDM7A-DT expression is correlated with highly aggressive cancer types and specific inherently determined subtypes (such as ductal invasive breast carcinoma (BRCA) basal subtype). Its regulation is determined by missense TP53 mutations in a subtype-specific context. KDM7A-DT transcribes several intermediate-sized ncRNAs and a full-length transcript, exhibiting distinct expression and localization patterns. Overexpression of KDM7A-DT upregulates TP53 protein expression and H2AX phosphorylation in nonmalignant fibroblasts, while in semi-transformed fibroblasts, OS superinduces KDM7A-DT expression in a TP53-dependent manner. KDM7A-DT knockdown and gene expression profiling in TP53 -missense mutated luminal A BRCA variant, where it is abundantly expressed, indicate its significant role in cancer pathways. Endogenous over-expression of KDM7A-DT inhibits DNA damage response/repair (DDR/R) via the TP53BP1-mediated pathway, reducing apoptosis and promoting G2/M checkpoint arrest. Higher KDM7A-DT expression in BRCA is associated with KDM7A-DT locus gain/amplification, higher histologic grade, aneuploidy, hypoxia, immune modulation scores, and activation of the c-myc pathway. Higher KDM7A-DT expression is associated with relatively poor survival outcomes in patients with luminal A or Basal subtypes. In contrast, it is associated with favorable outcomes in patients with HER2+ER- or luminal B subtypes. KDM7A-DT levels are coregulated with critical transcripts and proteins aberrantly expressed in BRCA, including those involved in DNA repair via non-homologous end joining and epithelial-to-mesenchymal transition pathway. In summary, KDM7A-DT and its si-lncRNA exhibit several intrinsic biological and clinical characteristics that suggest important roles in invasive BRCA and its subtypes. KDM7A-DT -defined mRNA and protein subnetworks offer resources for identifying clinically relevant RNA-based signatures and prospective targets for therapeutic intervention.
May 2024
·
17 Reads
Although KRAS G12C inhibitors have proven that KRAS is a “druggable” target of cancer, KRAS G12C inhibitor monotherapies have demonstrated limited clinical efficacy due to primary and acquired resistance mechanisms. Multiple combinations of KRAS G12C inhibitors with other targeted therapies, such as RTK, SHP2, and MEK inhibitors, have been investigated in clinical trials to overcome the resistance. They have demonstrated promising efficacy especially by combining KRAS G12C and EGFR inhibitors for KRAS G12C-mutated colorectal cancer. Many clinical trials of combinations of KRAS G12C inhibitors with other targeted therapies, such as SOS1, ERK, CDK4/6, and wild-type RAS, are ongoing. Furthermore, preclinical data have suggested additional promising KRAS G12C combinations with YAP/TAZ-TEAD inhibitors, FAK inhibitors, and farnesyltransferase inhibitors. The combinations of KRAS G12C inhibitors with immunotherapies and chemotherapies have also been investigated, and the preliminary results were reported. More recently, KRAS-targeted therapies not limited to KRAS G12C are being developed, potentially broadening the treatment landscape of KRAS-mutated cancers. Rationally combining KRAS inhibitors with other therapeutics is likely to play a significant role in future treatment for KRAS-mutated solid tumors.
May 2024
·
2 Reads
Background The measurement of minimal residual disease (MRD) by multiparametric flow cytometry (MFC) before hematopoietic stem cell transplantation (HSCT) in patients with acute myeloid leukemia (AML) is a powerful prognostic factor. The interaction of pretransplant MRD and the conditioning intensity has not yet been clarified. Objective The aim of this study is to analyze the transplant outcomes of patients with AML who underwent HSCT in complete remission (CR), comparing patients with positive MRD (MRD+) and negative MRD (MRD−) before HSCT, and the interaction between conditioning intensity and pre-HSCT MRD. Study design We retrospectively analyzed the transplant outcomes of 118 patients with AML who underwent HSCT in CR in a single institution, comparing patients with MRD+ and MRD− before HSCT using a cutoff of 0.1% on MFC, and the interaction between conditioning intensity and pre-HSCT MRD. Results Patients with MRD+ before HSCT had a significantly worse 2-year (2y) event-free survival (EFS) (56.5% vs. 32.0%, p = 0.018) than MRD− patients, due to a higher cumulative incidence of relapse (CIR) at 2 years (49.0% vs. 18.0%, p = 0.002), with no differences in transplant-related mortality (TRM) (2y-TRM, 19.0% and 25.0%, respectively, p = 0.588). In the analysis stratified by conditioning intensity, in patients who received MAC, those with MRD− before HSCT had better EFS ( p = 0.009) and overall survival (OS) ( p = 0.070) due to lower CIR ( p = 0.004) than MRD+ patients. On the other hand, the survival was similar in reduced intensity conditioning (RIC) patients regardless of the MRD status. Conclusions Patients with MRD+ before HSCT have worse outcomes than MRD− patients. In patients who received MAC, MRD− patients have better EFS and OS due to lower CIR than MRD+ patients, probably because they represent a more chemo-sensitive group. However, among RIC patients, results were similar regardless of the MRD status.
May 2024
·
1 Read
Chengli Wang
·
Liling Lin
·
Jiayao Wu
·
[...]
·
Minghui Cao
Background The aim of the present study was to build and internally validate a nomogram model for predicting prolonged length of stay (PLOS) among patients receiving free vascularized flap reconstruction of head and neck cancer (HNC). Methods A retrospective clinical study was performed at a single center, examining patients receiving free vascularized flap reconstruction of HNC from January 2011 to January 2019. The variables were obtained from the electronic information system. The primary outcome measure was PLOS. Univariate and multivariate analyses were used to find risk factors for predicting PLOS. A model was then built according to multivariate results. Internal validation was implemented via 1000 bootstrap samples. Results The study included 1047 patients, and the median length of stay (LOS) was 13.00 (11.00, 16.00) days. Multivariate analysis showed that flap types ((radial forearm free flap (odds ratio [OR] = 2.238; 95% CI, 1.403-3.569; P = 0.001), free fibula flap (OR = 3.319; 95% CI, 2.019-4.882; P < 0.001)), duration of surgery (OR = 1.002; 95% CI, 1.001-1.003; P = 0.004), postoperative complications (OR = 0.205; 95% CI, 0.129-0.325; P = P < 0.001) and unplanned reoperation (OR = 0.303; 95% CI, 0.140-0.653; P = 0.002) were associated with PLOS. In addition to these variables, blood transfusion was comprised in the model. The AUC of the model was 0.78 (95% CI, 0.711–0.849) and 0.725 (95% CI, 0.605–0.845) in the primary and internal validation cohorts, respectively. The DCA revealed the clinical utility of the current model when making intervention decisions within the PLOS possibility threshold range of 0.2-0.8. Conclusions Our study developed a nomogram that exhibits a commendable level of accuracy, thereby aiding clinicians in assessing the risk of PLOS among patients receiving free vascularized flap reconstruction for HNC.


May 2024
·
1 Read
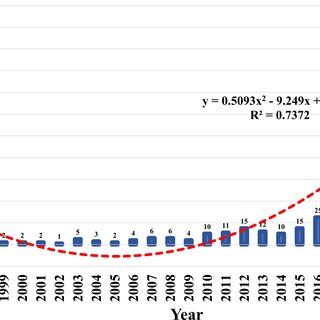
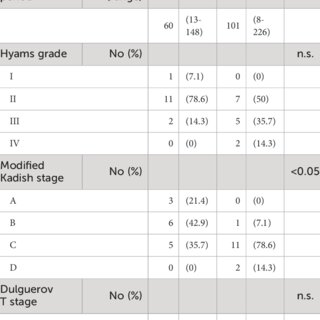
Background Olfactory neuroblastoma (ONB) is a rare malignant tumor arising from the olfactory neuroepithelium. The standard of care for ONB is surgical resection; however, detailed treatment protocols vary by institution. Our treatment protocol consists of endoscopic skull base surgery (ESBS) for endoscopically resectable cases and induction chemotherapy followed by craniotomy combined with ESBS for locally advanced cases, with postoperative radiotherapy performed for all cases. Chemoradiotherapy (CRT) is performed in unresectable cases. In this study, we evaluate our treatment protocol and outcomes for ONB. Methods A retrospective review of patients with ONB was conducted. Outcomes included survival outcomes and perioperative data. Results Fifteen patients (53.6%) underwent ESBS, 12 (42.9%) underwent craniotomy combined with ESBS, and 1 (3.6%) received CRT. The 5- and 10-year overall survival rates for all patients were 92.9% and 82.5%, respectively, with a median follow-up period of 81 months. The 5- and 10-year disease-free survival rates were 77.3% and 70.3%, respectively, and the 5- and 10-year local control rates were 88.2% and 80.2%, respectively. Patients undergoing ESBS demonstrated a significantly shorter operating time, period from operation to ambulation, hospitalization period, and less blood loss than those undergoing craniotomy combined with ESBS. Conclusion Our treatment protocol was found to afford favorable outcomes. Patients who underwent endoscopic resection showed lower complication rates and better perioperative data than those who underwent craniotomy combined with ESBS. With appropriate case selection, ESBS is considered a useful approach for ONB.
May 2024
April 2024




April 2024
·
3 Reads
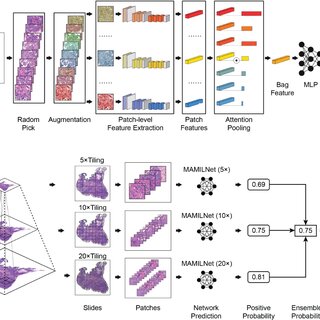
Background Whole Slide Image (WSI) analysis, driven by deep learning algorithms, has the potential to revolutionize tumor detection, classification, and treatment response prediction. However, challenges persist, such as limited model generalizability across various cancer types, the labor-intensive nature of patch-level annotation, and the necessity of integrating multi-magnification information to attain a comprehensive understanding of pathological patterns. Methods In response to these challenges, we introduce MAMILNet, an innovative multi-scale attentional multi-instance learning framework for WSI analysis. The incorporation of attention mechanisms into MAMILNet contributes to its exceptional generalizability across diverse cancer types and prediction tasks. This model considers whole slides as “bags” and individual patches as “instances.” By adopting this approach, MAMILNet effectively eliminates the requirement for intricate patch-level labeling, significantly reducing the manual workload for pathologists. To enhance prediction accuracy, the model employs a multi-scale “consultation” strategy, facilitating the aggregation of test outcomes from various magnifications. Results Our assessment of MAMILNet encompasses 1171 cases encompassing a wide range of cancer types, showcasing its effectiveness in predicting complex tasks. Remarkably, MAMILNet achieved impressive results in distinct domains: for breast cancer tumor detection, the Area Under the Curve (AUC) was 0.8872, with an Accuracy of 0.8760. In the realm of lung cancer typing diagnosis, it achieved an AUC of 0.9551 and an Accuracy of 0.9095. Furthermore, in predicting drug therapy responses for ovarian cancer, MAMILNet achieved an AUC of 0.7358 and an Accuracy of 0.7341. Conclusion The outcomes of this study underscore the potential of MAMILNet in driving the advancement of precision medicine and individualized treatment planning within the field of oncology. By effectively addressing challenges related to model generalization, annotation workload, and multi-magnification integration, MAMILNet shows promise in enhancing healthcare outcomes for cancer patients. The framework’s success in accurately detecting breast tumors, diagnosing lung cancer types, and predicting ovarian cancer therapy responses highlights its significant contribution to the field and paves the way for improved patient care.




April 2024
·
19 Reads
Objectives: This manuscript presents a bibliometric and visualization analysis of Total Body Irradiation (TBI) research, aiming to elucidate trends, gaps, and future directions in the field. This study aims to provide a comprehensive overview of the global research landscape of TBI, highlighting its key contributions, evolving trends, and potential areas for future exploration. Methods: The data for this study were extracted from the Web of Science Core Collection (WoSCC), encompassing articles published up to May 2023. The analysis included original studies, abstracts, and review articles focusing on TBI-related research. Bibliometric indicators such as total publications (TP), total citations (TC), and citations per publication (C/P) were utilized to assess the research output and impact. Visualization tools such as VOS Viewer were employed for thematic mapping and to illustrate international collaboration networks. Results: The analysis revealed a substantial body of literature, with 7,315 articles published by 2,650 institutions involving, 13,979 authors. Full-length articles were predominant, highlighting their central role in the dissemination of TBI research. The authorship pattern indicated a diverse range of scholarly influences, with both established and emerging researchers contributing significantly. The USA led in global contributions, with significant international collaborations observed. Recent research trends have focused on refining TBI treatment techniques, investigating long-term patient effects, and advancing dosimetry and biomarker studies for radiation exposure assessments. Conclusions: TBI research exhibits a dynamic and multifaceted landscape, driven by global collaboration and innovation. It highlights the clinical challenges of TBI, such as its adverse effects and the need for tailored treatments in pediatric cases. Crucially, the study also acknowledges the fundamental science underpinning TBI, including its effects on inflammatory and apoptotic pathways, DNA damage, and the varied sensitivity of cells and tissues. This dual focus enhances our understanding of TBI, guiding future research toward innovative solutions and comprehensive care


April 2024
·
3 Reads
The core of tumor cell metabolism is the management of energy metabolism due to the extremely high energy requirements of tumor cells. The purine nucleotide synthesis pathway in cells uses the purinosomes as an essential spatial structural complex. In addition to serving a crucial regulatory role in the emergence and growth of tumors, it contributes to the synthesis and metabolism of purine nucleotides. The significance of purine metabolism in tumor cells is initially addressed in this current article. The role of purinosomes as prospective therapeutic targets is then reviewed, along with a list of the signaling pathways that play in the regulation of tumor metabolism. A thorough comprehension of the function of purinosomes in the control of tumor metabolism can generate fresh suggestions for the creation of innovative cancer treatment methods.
April 2024
·
20 Reads
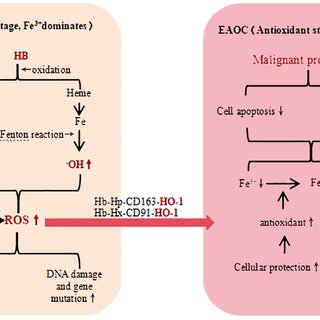
Endometriosis-associated ovarian cancer (EAOC) is a unique subtype of ovarian malignant tumor originating from endometriosis (EMS) malignant transformation, which has gradually become one of the hot topics in clinical and basic research in recent years. According to clinicopathological and epidemiological findings, precancerous lesions of ovarian clear cell carcinoma (OCCC) and ovarian endometrioid carcinoma (OEC) are considered as EMS. Given the large number of patients with endometriosis and its long time window for malignant transformation, sufficient attention should be paid to EAOC. At present, the pathogenesis of EAOC has not been clarified, no reliable biomarkers have been found in the diagnosis, and there is still a lack of basis and targets for stratified management and precise treatment in the treatment. At the same time, due to the long medical history of patients, the fast growth rate of cancer cells, and the possibility of eliminating the earliest endometriosis-associated ovarian cancer, it is difficult to find the corresponding histological evidence. As a result, few patients are finally diagnosed with EAOC, which increases the difficulty of in-depth study of EAOC. This article reviews the epidemiology, pathogenesis, risk factors, clinical diagnosis, new treatment strategies and prognosis of endometriosis-associated ovarian cancer, and prospects the future direction of basic research and clinical transformation, in order to achieve stratified management and personalized treatment of ovarian cancer patients.


April 2024
·
14 Reads
Sebastián Aguiar-Rosas·
 Ricardo Plancarte-Sánchez
Ricardo Plancarte-Sánchez·
 Carolina Hernández-Porras
Carolina Hernández-Porras·
[...]
·
Silvia Alarcón-BarriosCervical cancer (CC) occupies the second place in incidence and mortality among women in México. Despite this, Cervical Cancer continues to have a late diagnosis which leads to a high rate of complications. Pain represents the most feared and disabling symptom, being present in up to 86% of patients with advanced disease. The approach to managing pain in this population has not been studied and described to a full extent. In addition, there is a pressing need to provide concise recommendations to promote adequate pain control. We performed a review of the literature in CC and had experts in the field of pain management evaluate the evidence found. We then issued relevant recommendations on pharmacology and interventional pain management. Thus, the approach to pain management must be comprehensive and individualized, considering the timely and appropriate use of pharmacologic treatment as well as interventional procedures.



April 2024
·
24 Reads
Background Lynch syndrome (LS) is an autosomal dominant multi-organ cancer syndrome with a high lifetime risk of cancer. The number of cumulative colorectal adenomas in LS does not generally exceed ten, and removal of adenomas via routine screening minimizes the cancer burden. However, abnormal phenotypes may mislead initial diagnosis and subsequently cause suboptimal treatment. Aim Currently, there is no standard guide for the care of multiple colorectal adenomas in LS individuals. We aimed to shed insight into the molecular features and reasons for multiplicity of adenomas in LS patients. Methods We applied whole exome sequencing on nine adenomas (ten samples) and three assumed primary carcinomas (five samples) of an LS patient developing the tumors during a 21-year follow-up period. We compared the findings to the tumor profiles of two additional LS cases ascertained through colorectal tumor multiplicity, as well as to ten adenomas and 15 carcinomas from 23 unrelated LS patients with no elevated adenoma burden from the same population. As LS associated cancers can arise via several molecular pathways, we also profiled the tumors for CpG Island Methylator Phenotype (CIMP), and LINE-1 methylation. Results All tumors were microsatellite unstable (MSI), and MSI was present in several samples derived from normal mucosa as well. Interestingly, frequent frameshift variants in RNF43 were shared among substantial number of the tumors of our primary case and the tumors of LS cases with multiple tumors but almost absent in our control LS cases. The RNF43 variants were completely absent in the normal tissue, indicating tumor-associated mutational hotspots. The RNF43 status correlated with the mutational signature SBS96. Contrary to LS tumors from the reference set with no elevated colorectal tumor burden, the somatic variants occurred significantly more frequently at C>T in the CpG context, irrespective of CIMP or LINE-1 status, potentially indicating other, yet unknown methylation-related mechanisms. There were no signs of somatic mosaicism affecting the MMR genes. Somatic variants in APC and CTNNB1 were unique to each tumor. Conclusion Frequent somatic RNF43 hot spot variants combined with SBS96 signature and increased tendency to DNA methylation may contribute to tumor multiplicity in LS.



April 2024
·
30 Reads
BReast CAncer ( BRCA )1 and BRCA2 gene pathogenic variants account for most hereditary breast cancers (BC). Identification of BRCA mutations can significantly influence both prognosis and treatment outcomes. Furthermore, it enables the identification of individuals who are at heightened risk of developing BC due to inherited genetic mutations. Many developing countries rely on western guidelines for BRCA testing and BC management; however, there exist wide disparities in the prevalence of risk factors, availability of medical resources, and practice patterns. Guidelines tailored to specific regions can help mitigate healthcare variations, promote consistency in treatment, and aid healthcare providers in identifying effective therapies for improving patient outcomes. Hence, oncologists from the Gulf Cooperation Council (GCC) congregated virtually in March 2023 and reviewed existing data on the epidemiology of BC, BRCA mutations, practices and challenges associated with BRCA testing and management of BRCA mutated early-stage BC in the GCC region. They also provided insights on the real-world diagnostic and treatment practices and challenges in the GCC region in the BRCA -mutated early-stage BC domain and suggested some variations to international guidelines to aid their uptake in this region.
April 2024
·
14 Reads
Introduction Women living with human immunodeficiency virus (WLHIV) face elevated risks of human papillomavirus (HPV) acquisition and cervical cancer (CC). Coverage of CC screening and treatment remains low in low-and-middle-income settings, reflecting resource challenges and loss to follow-up with current strategies. We estimated the health and economic impact of alternative scalable CC screening strategies in KwaZulu-Natal, South Africa, a region with high burden of CC and HIV. Methods We parameterized a dynamic compartmental model of HPV and HIV transmission and CC natural history to KwaZulu-Natal. Over 100 years, we simulated the status quo of a multi-visit screening and treatment strategy with cytology and colposcopy triage (South African standard of care) and six single-visit comparator scenarios with varying: 1) screening strategy (HPV DNA testing alone, with genotyping, or with automated visual evaluation triage, a new high-performance technology), 2) screening frequency (once-per-lifetime for all women, or repeated every 5 years for WLHIV and twice for women without HIV), and 3) loss to follow-up for treatment. Using the Ministry of Health perspective, we estimated costs associated with HPV vaccination, screening, and pre-cancer, CC, and HIV treatment. We quantified CC cases, deaths, and disability-adjusted life-years (DALYs) averted for each scenario. We discounted costs (2022 US dollars) and outcomes at 3% annually and calculated incremental cost-effectiveness ratios (ICERs). Results We projected 69,294 new CC cases and 43,950 CC-related deaths in the status quo scenario. HPV DNA testing achieved the greatest improvement in health outcomes, averting 9.4% of cases and 9.0% of deaths with one-time screening and 37.1% and 35.1%, respectively, with repeat screening. Compared to the cost of the status quo ($12.79 billion), repeat screening using HPV DNA genotyping had the greatest increase in costs. Repeat screening with HPV DNA testing was the most effective strategy below the willingness to pay threshold (ICER: $3,194/DALY averted). One-time screening with HPV DNA testing was also an efficient strategy (ICER: $1,398/DALY averted). Conclusions Repeat single-visit screening with HPV DNA testing was the optimal strategy simulated. Single-visit strategies with increased frequency for WLHIV may be cost-effective in KwaZulu-Natal and similar settings with high HIV and HPV prevalence.
April 2024
Purpose This study aims to evaluate the efficacy and safety of ultrasound-guided percutaneous biopsy of the first hepatic hilum lesion, and examine its clinical value of diagnosis and treatment. Methods We conducted a retrospective study on patients diagnosed with the first hepatic hilum lesions at Fujian Provincial Hospital between February 2015 and October 2022. We selected patients who had lesions in the first hepatic hilum(including a 2cm surrounding area of the left/right hepatic ducts and upper-middle segment of the common bile duct) and the liver periphery(in the peripheral area of the liver, outside of the above-mentioned first hepatic porta region). These patients underwent percutaneous ultrasound-guided core needle biopsy (PUS-CNB) with cognitive fusion guidance using CT, MRI, or PET-CT. We compared the safety and efficacy of PUS-CNB in the first hepatic hilum and the liver periphery to explore the value of PUS-CNB in optimizing the clinical treatment of the first hepatic hilum lesions. Results The studied includes 38 cases of the first hepatic hilum cases (18 females; 20 males), 23 presented with mass-forming tumors while the remaining 15 exhibited diffuse infiltrative tumors, with an average diameter of 4.65± 2.51 cm. The percutaneous biopsy procedure, conducted under ultrasound guidance, had an average operation time of 14.55 ± 2.73 minutes, and resulted in a postoperative bleeding volume of approximately 10.79 ± 2.79 ml. The diagnostic success rate was noted to be as high as 92.11% among the participants who underwent percutaneous biopsy of the first hepatic hilum. Procedural complications, such as bleeding, bile leakage, intestinal perforation, infection or needle tract seeding, did not occur during or after the biopsy procedure. Affected by biopsy results, 5 altered their clinical treatment plans accordingly, 24patients received non-surgical treatment, 9 underwent surgical treatment, 5 underwent radiofrequency ablation for the lesions. The study comprised a total of 112 cases for percutaneous biopsy of the liver periphery. The safety and effectiveness of the two biopsy techniques were comparable, with diagnostic success rates of 92.11% VS. 94.34%, respectively ( p = 0.61). Conclusion Cognitive fusion of ultrasound and multi-modal imaging for the first hepatic hilum lesion puncture biopsy is a safe and effective diagnostic procedure, with better diagnostic rate, may improve clinical value of diagnosis and treatment of various diseases.
![FIGURE 1 Histopathology and immunohistochemistry (IHC) of HNSC. (A, B) H&E stain, original magnification ×100,×400. (C) IHC CK(pan)(+) original magnification ×200. (D) IHC Vimentin(+), original magnification ×200. (E) IHC GATA3(+) original magnification ×20. (F) IHC Melan(+) original magnification ×20. (G) PD-L1 IHC (Dako22C3), original magnification ×40. Combined Positive Score [CPS]: 95. (CPS was defined as the number of PD-L1 stained cells (tumor cells, lymphocytes, macrophages) divided by the number of all tumor cells and multiplied by 100.).](https://www.researchgate.net/publication/380123232/figure/fig2/AS:11431281239043588@1714142295686/Histopathology-and-immunohistochemistry-IHC-of-HNSC-A-B-H-E-stain-original_Q320.jpg)


April 2024
·
3 Reads
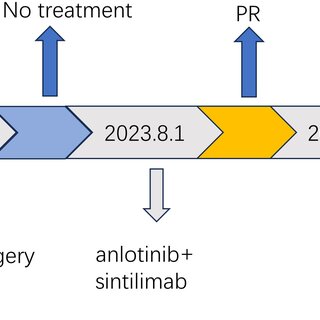
Sarcomatoid carcinoma (SC) is a rare, complex, aggressive tumor that spreads rapidly, is highly malignant, and has metastasized. Surgical resection is the primary treatment, and it usually occurs in the lungs and kidneys but rarely in the neck. Patients with advanced sarcomatoid carcinoma (SC) of the head and neck (HN) have a poor progonsis. In recent years, immune checkpoint inhibitors (ICIs) have been established as treatments for many solid tumors; however, the effectiveness of ICIs in treating SC of HN is still little recognized. We report a case study of a middle-aged woman with primary sarcomatoid carcinoma of the neck. She developed sarcomatoid carcinoma of the contralateral neck 7 months after the first surgical treatment. Subsequently, disease recurrence and metastasis occurred 8 months after the second surgery. The patient did not receive any treatment after both surgeries. The tumor showed high programmed death-ligand 1 (PD-L1) expression, with a combined positive score (CPS): 95. The patient’s response to treatment was assessed as partial remission (PR) after 2 cycles of anlotinib combined with sintilimab. The patient has survived for over 2 years and remains in PR status, despite experiencing grade 2 hypothyroidism as an adverse event during treatment. The case highlights the efficacy and safety of anlotinib and sintilimab as a first-line treatment.




April 2024
·
38 Reads
Background Molecular testing plays a pivotal role in monitoring measurable residual disease (MRD) in acute myeloid leukemia (AML), aiding in the refinement of risk stratification and treatment guidance. Wilms tumor gene 1 ( WT1 ) is frequently upregulated in pediatric AML and serves as a potential molecular marker for MRD. This study aimed to evaluate WT1 predictive value as an MRD marker and its impact on disease prognosis. Methods Quantification of WT1 expression levels was analyzed using the standardized European Leukemia Network real-time quantitative polymerase chain reaction assay (qRT-PCR) among a cohort of 146 pediatric AML patients. Post-induction I and intensification I, MRD response by WT1 was assessed. Patients achieving a ≥2 log reduction in WT1 MRD were categorized as good responders, while those failing to reach this threshold were classified as poor responders. Results At diagnosis, WT1 overexpression was observed in 112 out of 146 (76.7%) patients. Significantly high levels were found in patients with M4- FAB subtype (p=0.018) and core binding fusion transcript (CBF) ( RUNX1::RUNX1T1 , p=0.018, CBFB::MYH11 , p=0.016). Following induction treatment, good responders exhibited a reduced risk of relapse (2-year cumulative incidence of relapse [CIR] 7.9% vs 33.2%, p=0.008). Conversely, poor responders’ post-intensification I showed significantly lower overall survival (OS) (51% vs 93.2%, p<0.001), event-free survival (EFS) (33.3% vs 82.6%, p<0.001), and higher CIR (66.6% vs 10.6%, p<0.001) at 24 months compared to good responders. Even after adjusting for potential confounders, it remained an independent adverse prognostic factor for OS (p=0.04) and EFS (p=0.008). High concordance rates between WT1 -based MRD response and molecular MRD were observed in CBF patients. Furthermore, failure to achieve either a 3-log reduction by RT-PCR or a 2-log reduction by WT1 indicated a high risk of relapse. Combining MFC-based and WT1 -based MRD results among the intermediate-risk group identified patients with unfavorable prognosis (positive predictive value [PPV] 100%, negative predictive value [NPV] 85%, and accuracy 87.5%). Conclusion WT1 MRD response post-intensification I serves as an independent prognostic factor for survival in pediatric AML. Integration of WT1 and MFC-based MRD results enhances the reliability of MRD-based prognostic stratification, particularly in patients lacking specific leukemic markers, thereby influencing treatment strategies.




April 2024
·
5 Reads
Background Elderly patients diagnosed with diffuse large B-cell lymphoma (DLBCL) undergoing reduced intensity R-CHOP therapy are at a heightened risk of acquiring infections, notably coronavirus disease 2019 (COVID-19) infection. This study aimed to evaluate the efficacy of intravenous immunoglobulin (IVIG) as prophylaxis against COVID-19 in this vulnerable population. Methods A total of 125 elderly patients with DLBCL undergoing reduced intensity R-CHOP therapy were analyzed in this prospective, multicenter study. Patients with hypogammaglobulinemia were categorized into IVIG and non-IVIG groups, while those with normal immunoglobulin levels constituted the observation group. The study evaluated COVID-19 infection rates, therapy response, and safety outcomes. Results Among the enrolled patients (median age: 77 years), 89 patients (71.2%) presented with hypogammaglobulinemia at diagnosis, and 56 patients enrolled in the IVIG administration group. IVIG administration remarkably reduced COVID-19 infection rates compared to non-IVIG recipients (8.9% vs. 24.6%; p =0.040). Notably, patients over 80 years old were more susceptible to COVID-19. Patients on IVIG exhibited good tolerance with manageable adverse events. Among patients with hypogammaglobulinemia who received IVIG, 40.5% of patients developed additional immunoglobulin deficiencies during chemotherapy. One or more new hypogammaglobulinemia occurred during chemotherapy in 72% of patients with hypogammaglobulinemia who did not receive IVIG, and in 61.3% of patients who did not have hypogammaglobulinemia at diagnosis. Conclusion IVIG showed promise in reducing COVID-19 infections among elderly patients with DLBCL receiving reduced intensity R-CHOP therapy. This highlights IVIG’s potential as a prophylactic measure, necessitating further investigation to optimize dosing, administration schedules, and potential interactions with vaccination strategies.




April 2024
·
3 Reads
Background As circulating tumour DNA (ctDNA) liquid biopsy analysis is increasingly incorporated into modern oncological practice, establishing the impact of genomic intra-tumoural heterogeneity (ITH) upon data output is paramount. Despite advances in other cancer types the evidence base in head and neck squamous cell carcinoma (HNSCC) remains poor. We sought to investigate the utility of ctDNA to detect ITH in HNSCC. Methods In a pilot cohort of 9 treatment-naïve HNSCC patients, DNA from two intra-tumoural sites (core and margin) was whole-exome sequenced. A 9-gene panel was designed to perform targeted sequencing on pre-treatment plasma cell-free DNA and selected post-treatment samples. Results Rates of genomic ITH among the 9 patients was high. COSMIC variants from 19 TCGA HNSCC genes demonstrated an 86.9% heterogeneity rate (present in one tumour sub-site only). Across all patients, cell-free DNA (ctDNA) identified 12.9% (range 7.5-19.8%) of tumour-specific variants, of which 55.6% were specific to a single tumour sub-site only. CtDNA identified 79.0% (range: 55.6-90.9%) of high-frequency variants (tumour VAF>5%). Analysis of ctDNA in serial post-treatment blood samples in patients who suffered recurrence demonstrated dynamic changes in both tumour-specific and acquired variants that predicted recurrence ahead of clinical detection. Conclusion We demonstrate that a ctDNA liquid biopsy identified spatial genomic ITH in HNSCC and reliably detected high-frequency driver mutations. Serial sampling allowed post-treatment surveillance and early identification of treatment failure.




April 2024
·
20 Reads
The main known function of Nudix hydrolase 2 (Nudt2) is to hydrolyze the secondary messenger diadenosine 5’, 5’’’-p1, p4-tetraphosphate (Ap4A). In this study we examined the role of Nudt2 in breast carcinoma through its expression in human invasive ductal carcinoma tissues, and its functions in human triple negative breast cancer (TNBC) cell lines. A significantly higher expression of Nudt2 was observed in human invasive ductal carcinoma tissues compared to that in normal breast tissue. Knockdown of Nudt2 in TNBC cell lines resulted in a significant reduction in cellular proliferation via the Ki67 marker, accompanied by G0/G1 phase cell cycle arrest, in the migration and invasion of these cells and in tumorigenicity and anchorage-independent growth. It can therefore be concluded that Nudt2 plays a significant role in promoting TNBC growth.

April 2024
·
8 Reads
Routine use of human papillomavirus (HPV) vaccines is recommended in adolescents under 15 years of age worldwide. Still, effective programs remain suboptimal for several factors, making the WHO strategy to eradicate cervical cancer public health with an uncertain future. Objective To review the literature on the effectiveness, long-term protection, and safety of HPV vaccination programs and vaccination as adjuvant management. This review aims to describe the current state of vaccination programs and demonstrate the long-term protection and safety of vaccines implemented worldwide targeting adolescent girls, with the most recent published evidence of the three prophylactic HPV vaccines – bivalent (bHPV), quadrivalent (qHPV), and nonavalent (nHPV)-. We mainly focus on publications evaluating efficacy, dosing schemes, and HPV vaccination, as well as studies contributing to the mounting evidence for the real-life effectiveness of prophylactic HPV vaccines from several countries. Findings Human Papillomavirus vaccination programs have made remarkable strides in preventing HPV-related diseases; countries with robust vaccination efforts have witnessed substantial reductions in HPV-related diseases with a decline in high-grade cervical abnormalities and genital warts (54%-83%). However, global coverage remains uneven, with disparities between high-income (HICs) and low-income countries (LMICs). The long-term efficacy of the available human papillomavirus (HPV) goes up to 9.4 years and continues to be immunogenic and well tolerated with an excellent safety profile. Conclusions and relevance As these are crucial topics in HPV vaccination, it is essential to establish systems for continued monitoring of vaccine immunogenicity, efficacy, and safety over time.




April 2024
·
3 Reads
Background Accurate detection of the histological grade of pancreatic neuroendocrine tumors (PNETs) is important for patients’ prognoses and treatment. Here, we investigated the performance of radiological image-based artificial intelligence (AI) models in predicting histological grades using meta-analysis. Method A systematic literature search was performed for studies published before September 2023. Study characteristics and diagnostic measures were extracted. Estimates were pooled using random-effects meta-analysis. Evaluation of risk of bias was performed by the QUADAS-2 tool. Results A total of 26 studies were included, 20 of which met the meta-analysis criteria. We found that the AI-based models had high area under the curve (AUC) values and showed moderate predictive value. The pooled distinguishing abilities between different grades of PNETs were 0.89 [0.84-0.90]. By performing subgroup analysis, we found that the radiomics feature-only models had a predictive value of 0.90 [0.87-0.92] with I ² = 89.91%, while the pooled AUC value of the combined group was 0.81 [0.77-0.84] with I ² = 41.54%. The validation group had a pooled AUC of 0.84 [0.81-0.87] without heterogenicity, whereas the validation-free group had high heterogenicity (I 2 = 91.65%, P=0.000). The machine learning group had a pooled AUC of 0.83 [0.80-0.86] with I ² = 82.28%. Conclusion AI can be considered as a potential tool to detect histological PNETs grades. Sample diversity, lack of external validation, imaging modalities, inconsistent radiomics feature extraction across platforms, different modeling algorithms and software choices were sources of heterogeneity. Standardized imaging, transparent statistical methodologies for feature selection and model development are still needed in the future to achieve the transformation of radiomics results into clinical applications. Systematic Review Registration https://www.crd.york.ac.uk/prospero/ , identifier CRD42022341852.
April 2024
·
4 Reads





















































